| Program Name: | BadgerCare Plus and Medicaid | Handbook Area: | Nurses in Independent Practice | | 05/14/2024 | Prior Authorization : Forms and AttachmentsTopic #960 An Overview
Depending on the service being requested, most PA requests must be comprised of the following:
Topic #446 Attachments
In addition to the PA/RF, PA/HIAS1, or PA/DRF, a service-specific PA attachment must be submitted with each PA request. The PA attachment allows a provider to document the clinical information used to determine whether or not the standards of medical necessity are met for the requested service(s). Providers should include adequate information for ForwardHealth to make a reasonable judgment about the case.
ForwardHealth will scan each form with a barcode as it is received, which will allow greater efficiencies for processing PA requests. Topic #2083 Documentation Requirements - Private Duty Nursing
For PDN services, the PAL is responsible for submitting PA request and supporting documentation.
PALs requesting PA for PDN services are required to include the following with the PA/RF:
Private Duty Nursing Prior Authorization Acknowledgment
Agencies are required to submit a completed and signed Private Duty Nursing Prior Authorization Acknowledgment with all PA requests for PDN services. This form acknowledges that the member or the member's legal representative has read the POC and PA request.
Documenting Expected Hours on the PA/RF
Providers are required to indicate on the PA/RF the medically necessary number of PDN hours per day, the number of days per week, and the number of weeks. The total number of PDN hours requested on the PA/RF must be equal to or less than the number of hours ordered by the physician and indicated on the POC. Services by another provider, whether another home health agency, NIP, pediatric community care, personal care provider, or volunteer, must also be indicated on the POC. Topic #447 Obtaining Forms and Attachments
Providers may obtain paper versions of all PA forms and attachments. In addition, providers may download and complete most PA attachments from the ForwardHealth Portal.
Paper Forms
Paper versions of all PA forms and PA attachments are available by writing to ForwardHealth. Include a return address, the name of the form, the form number (if applicable), and mail the request to the following address:
ForwardHealth
Form Reorder
313 Blettner Blvd
Madison WI 53784
Providers may also call Provider Services to order paper copies of forms.
Downloadable Forms
Most PA attachments can be downloaded and printed in their original format from the Portal. Many forms are available in fillable PDF and fillable Microsoft Word formats.
Web PA Via the Portal
Certain providers may complete the PA/RF and PA attachments through the Portal. Providers may then print the PA/RF (and in some cases the PA attachment), and send the PA/RF, service-specific PA attachments, and any supporting documentation on paper by mail or fax to ForwardHealth. Topic #1107 Plan of Care
The PAL is required to attach a copy of the member's POC with requests for PA and amendments. The information requested in each element of the PA/CPA is required information to be included in the POC, but the use of the PA/CPA is voluntary. The POC must contain all of the required information as instructed on the PA/CPA instructions. Before providing services, each PDN provider sharing the case is required to obtain a copy of the POC for the effective certification period and maintain the POC in their records. Topic #448 Prior Authorization Request Form
The PA/RF is used by ForwardHealth and is mandatory for most providers when requesting PA. The PA/RF serves as the cover page of a PA request.
Providers are required to complete the basic provider, member, and service information on the PA/RF. Each PA request is assigned a unique ten-digit number. ForwardHealth remittance information will report to the provider the PA number used to process the claim for prior authorized services. Topic #1109 Prior Authorization Requests for Private Duty Nursing Services
A PA/RF is mandatory when the PAL requests PA for PDN services.
The total hours requested on the PA/RF cannot exceed the number of hours on the physician-signed POC. Topic #1108 Prior Authorization Request Form Completion Instructions for Private Duty Nursing
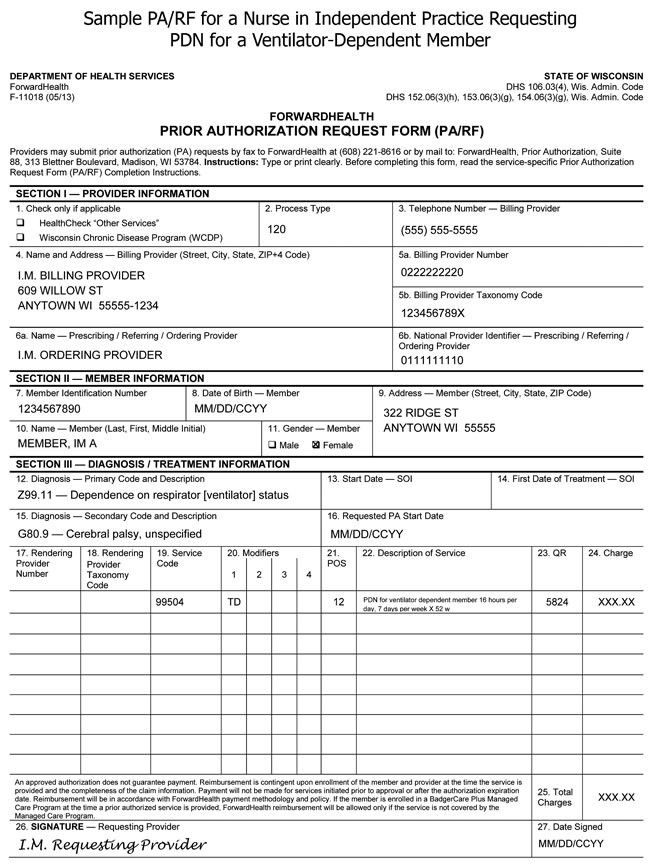
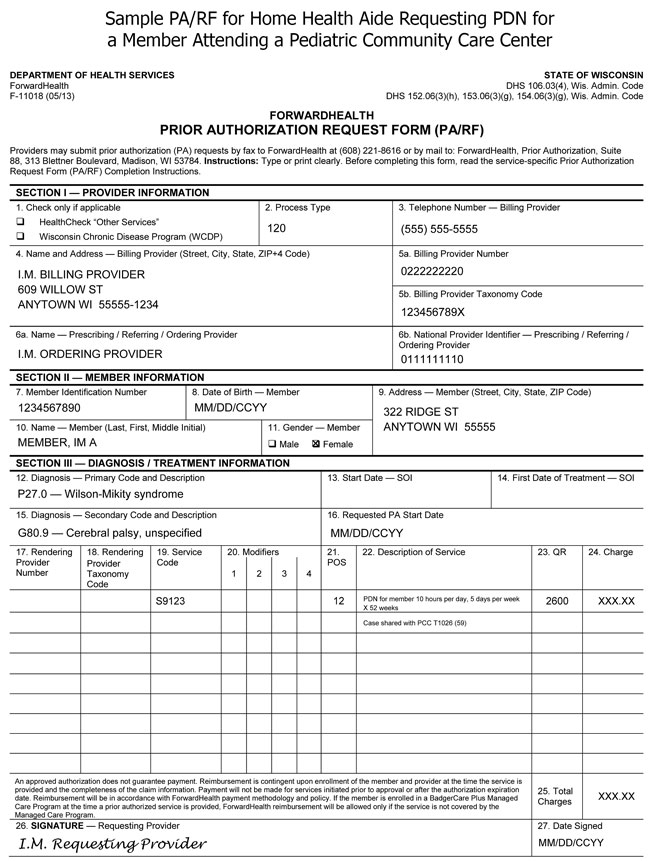
The following are sample PA/RFs for PDN services:
An NIP acting as the PDN PAL must indicate on the PA request the procedure code for the PDN services that the RN is to provide (S9123 or 99504 with modifier TD). When the PA request is adjudicated, ForwardHealth will add the corresponding procedure code (S9124 or 99504 with modifier TE) for PDN services that LPNs might provide.
For PA requests submitted by an NIP via the Portal for PDN services that include PDN services provided by PCC providers, the procedure code T1026 and modifier 59 must be included in the "Additional Service Code Description" field.
For paper PA requests submitted by an NIP by fax or by mail for PDN services that include PDN services provided by PCC providers, the procedure code T1026 and modifier 59 must be included in Element 21 (Description of Service). Refer to the sample PA/RF for PDN services requested by a PAL who is an NIP.
ForwardHealth requires certain information to enable the programs to authorize and pay for medical services provided to eligible members.
Members of ForwardHealth are required to give providers full, correct, and truthful information for the submission of correct and complete claims for reimbursement. This information should include, but is not limited to, information concerning enrollment status, accurate name, address, and member identification number (Wis. Admin. Code § DHS 104.02[4]).
Under Wis. Stat. § 49.45(4), personally identifiable information about program applicants and members is confidential and is used for purposes directly related to ForwardHealth administration such as determining eligibility of the applicant, processing PA requests, or processing provider claims for reimbursement. The use of the PA/RF is mandatory to receive PA for certain items. Failure to supply the information requested by the form may result in denial of PA or payment for the service.
Providers should retain copies of all paper documents mailed to ForwardHealth. Providers may submit PA requests, along with the POC containing no less information than is required for the PA/CPA and the Private Duty Nursing Prior Authorization Acknowledgment, via the ForwardHealth Portal, by fax to ForwardHealth at 608-221-8616, or by mail to the following address:
ForwardHealth
Prior Authorization
Ste 88
313 Blettner Blvd
Madison WI 53784
The provision of services that are greater than or significantly different
from those authorized may result in nonpayment of the billing claim(s).
SECTION I ― PROVIDER INFORMATION
Element 1 — HealthCheck "Other Services" and Wisconsin Chronic Disease
Program (WCDP)
Enter an "X" in the box next to HealthCheck "Other Services" if the
services requested on the PA/RF are for HealthCheck "Other Services." Enter an "X" in the box next to WCDP if the services requested on the PA/RF
are for a WCDP member.
Element 2 — Process Type
Enter process type "120" — PDN. The process type is used to identify a category of service requested. Prior authorization requests will be returned
without adjudication if no process type is indicated.
Element 3 — Telephone Number — Billing Provider
Enter the telephone number, including the area code, of the office, clinic,
facility, or place of business of the PAL.
Element 4 — Name and Address — Billing Provider
Enter the name and complete address (street, city, state, and ZIP+4 code)
of the PDN PAL. Providers are required to include both the ZIP code
and four-digit extension for timely and accurate billing. The name listed in
this element must correspond with the PDN PAL's number listed in
Element 5a.
Element 5a — Billing Provider Number
Enter the NPI of the PDN PAL. The
NPI in this element must correspond with the provider name listed in Element
4.
Element 5b — Billing Provider Taxonomy
Enter the national 10-digit alphanumeric taxonomy code that corresponds to
the PDN PAL's NPI in Element 5a.
Element 6a — Name — Prescribing/Referring/Ordering Provider
Enter the prescribing/referring/ordering provider's name.
Element 6b — National Provider Identifier — Prescribing/Referring/Ordering Provider
Enter the prescribing/referring/ordering provider's 10-digit NPI.
SECTION II ― MEMBER INFORMATION
Element 7 — Member Identification Number
Enter the member identification number. Do not enter any other numbers or
letters. Use the ForwardHealth identification card or Wisconsin's EVS to obtain the correct number.
Element 8 — Date of Birth — Member
Enter the member's date of birth in MM/DD/CCYY format (for example, September 8,
1966, would be 09/08/1966).
Element 9 — Address — Member
Enter the complete address of the member's place of residence, including
the street, city, state, and ZIP code.
Element 10 — Name — Member
Enter the member's last name, followed by their first name and middle
initial. Use the EVS to obtain the correct spelling of the member's name. If
the name or spelling of the name on the ForwardHealth card and the EVS do not
match, use the spelling from the EVS.
Element 11 — Gender — Member
Enter an "X" in the appropriate box to specify male or female.
SECTION III — DIAGNOSIS / TREATMENT INFORMATION
Element 12 — Diagnosis — Primary Code and Description
Enter the appropriate ICD diagnosis code and description with the highest level of specificity most
relevant to the service/procedure requested. The ICD diagnosis code must correspond with the ICD description.
Element 13 — Start Date — SOI (not required)
Element 14 — First Date of Treatment — SOI [not required]
Element 15 — Diagnosis — Secondary Code and Description
Enter the appropriate secondary ICD diagnosis code and description with the highest level of specificity most
relevant to the service/procedure requested, if applicable. The ICD diagnosis code must correspond with the ICD description.
Element 16 — Requested PA Start Date
Enter the requested start date for service(s) in MM/DD/CCYY format, if a
specific start date is requested.
Element 17 — Rendering Provider Number (not required)
Element 18 — Rendering Provider Taxonomy (not required)
Element 19 — Service Code
Enter the appropriate CPT code or HCPCS code for each service the PDN PAL will be providing.
When the PDN PAL is a NIP or a HHA, only the procedure code for PDN services that are provided by the RN should be placed in this element.
When the PDN PAL is a PCC provider, only the procedure code for the PDN services that are provided by the PCC provider should be placed in this element.
Note: If the provider needs additional spaces for Elements 18-23 for the PA
request, the provider may complete additional PA/RF(s). The PA/RFs should be
identified, for example, as "page 1 of 2" and "page 2 of 2."
Element 20 — Modifiers
Enter the appropriate modifier for the procedure code listed, as applicable
Element 21 — POS
Enter the appropriate POS code designating where the
requested service will be performed. Includes, but is not limited to, the following:
- 03 (School)
- 12 (Home)
- 99 (Other Place of Service)
Element 22 — Description of Service
For PDN services, the description of service must contain the following information:
- Enter a written description corresponding to the appropriate CPT or HCPCS code for the PDN services requested.
- Enter the number of hours per day, number of days per week, and the number of weeks being requested. (The total number of hours requested should not exceed the number of hours ordered by the physician on the POC).
Other information may be needed in the description of service for the following situations:
- When the PDN PAL is an NIP or an HHA and the member also attends a PCC program, the PDN PAL must enter the procedure code T1026 and modifier 59 for the PDN services that are provided by the PCC provider.
- When the PDN PAL is a PCC provider and the member also requests PDN services for times when they are not attending the PCC program, then the PCC PDN PAL must enter the procedure code and modifier (if needed) for the PDN services that are to be provided by an RN into this element (99504-TD for PDN for ventilator dependent members or S9123 for non-ventilator dependent members).
Element 23 — QR
Enter the appropriate quantity (for example, number of services) requested for the
procedure code listed.
Element 24 — Charge
Enter the usual and customary charge for each service requested.
Note: The charges indicated on the request form should reflect
the provider's usual and customary charge for the procedure requested.
Providers are reimbursed for authorized services according to the provider
Terms of Reimbursement issued by the Wisconsin DHS.
Element 25 — Total Charges
Enter the anticipated total charges for this request. If the provider
completed a multiple-page PA/RF, indicate the total charges for the entire PA
request on Element 22 of the last page of the PA/RF. On the preceding pages,
Element 22 should refer to the last page (for example, "SEE PAGE TWO").
Element 26 — Signature — Requesting Provider
The original signature of the provider requesting/performing/dispensing
this service/procedure/item must appear in this element.
Element 27 — Date Signed
Enter the month, day, and year the PA/RF was signed (in MM/DD/CCYY format).
Topic #1110 Private Duty Nursing Prior Authorization Acknowledgment
Wisconsin Medicaid requires the PDN PAL to submit a completed and signed Private Duty Nursing Prior Authorization Acknowledgment with all PA requests. This form acknowledges that the member or the member's legal representative has read the POC and PA request. Topic #1111 Required Documentation for Private Duty Nursing Prior Authorization Requests
The PAL is required to submit the following completed forms for PDN PA requests:
The PAL is required to make the PA request available for other PDN providers on the case to review. Topic #449 Supporting Clinical Documentation
Certain PA requests may require additional supporting clinical documentation to justify the medical necessity for a service(s). Supporting documentation may include, but is not limited to, X-rays, photographs, a physician's prescription, clinical reports, and other materials related to the member's condition.
All supporting documentation submitted with a PA request must be clearly labeled and identified with the member's name and member identification number. Securely packaged X-rays and dental models will be returned to providers.
Photographs submitted to ForwardHealth as additional supporting clinical documentation for PA requests will not be returned to providers and will be disposed of securely. Topic #14038 When a Home Health Agency is the Prior Authorization Liaison
PA requests for PDN services submitted by a home health agency should not include any procedure code for a service that is not PDN. Requests for PDN services combined with requests for other services will be returned to the provider.
Home health agencies acting as the PDN PAL must indicate on the PA request the procedure code for the PDN service that an RN is to provide (S9123 or 99504 with modifier TD). When the PA request is adjudicated, ForwardHealth will add the applicable corresponding procedure code for the PDN services an LPN might provide (S9124 or 99504 with modifier TE). If the PA request is authorized, the applicable procedure codes for PDN services will be stated in the PA decision notice letter.
For PA requests submitted by a home health agency via the Portal for PDN services that include PCC services, the procedure code T1026 with modifier 59 must be included in the "Additional Service Code Description" field.
For paper PA requests submitted by home health agency by fax or mail for PDN services that include PDN services provided by PCC providers, the procedure code T1026 and modifier 59 must be included in Element 21 (Description of Service). |